Approximately 30,000 people in the US are diagnosed with thoracic aortic aneurysms every year. Patients that experience the devastating event of rupture or dissection face up to 60% mortality.Currently, aTAA elective surgical repair is based primarily on aneurysm diameter or growth rate, with a ≥ 5.5cm diameter threshold for surgery in patients without connective tissue disorders or family history of dissection, rupture, or aneurysms.
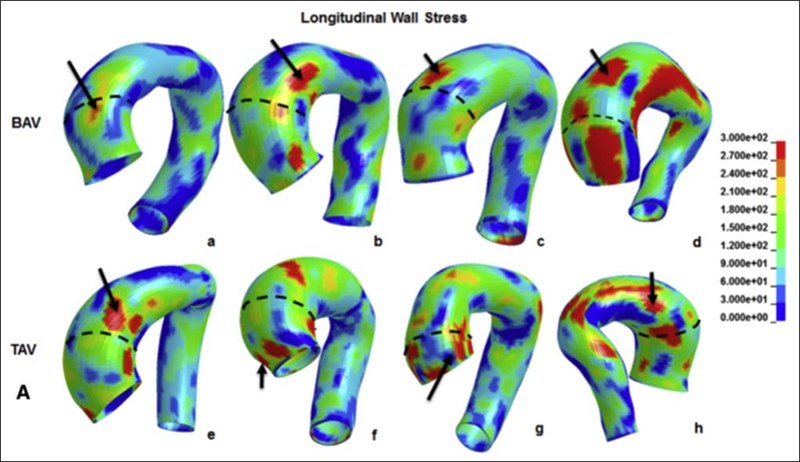
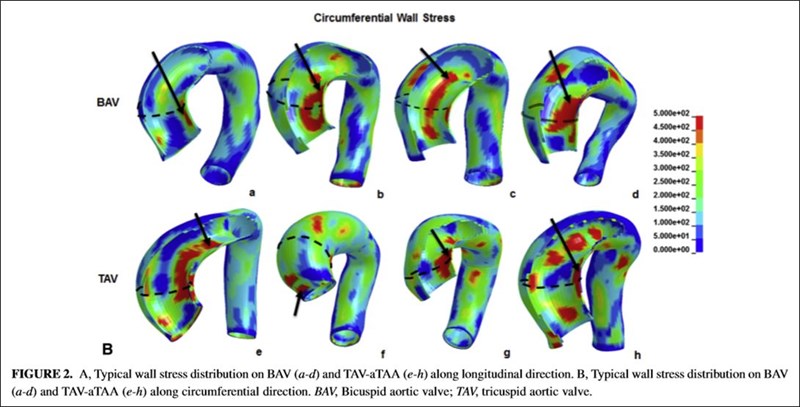
However, studies have demonstrated that a majority of aTAA rupture/dissection occurs in patients with aTAA diameters < 5.5cm. Alarmingly, significant numbers of patients are at risk for aortic dissection but have aTAA diameters under the cutoff for elective surgical intervention. Patient-specific aneurysm wall stresses determined from computational modeling holds great promise for elucidating patient-specific risk of aTAA dissection.
Goals
References
Xuan Y, Wang Z, Liu R, Haraldsson H, Hope MD, Saloner DA, Guccione JM, Ge L, Tseng E. Wall stress on ascending thoracic aortic aneurysms with bicuspid compared to tricuspid aortic valve. J Thorac Cardiovasc Surg 2018;156:492-500.